
24.09.2018
The Role of Inflammation
What is inflammation?
Inflammation is the response to a soft tissue injury that results in the release of inflammatory chemicals (known as inflammatory cytokines) into the tissue. These chemicals create an inflammatory cascade, seeing the infiltration of a variety of cells that, like most other cells, convert oxygen into energy (fuel) in order to work to clean up damaged tissue and others that build new tissue. Inflammation is the first important element of tissue healing where clotting occurs and cells are recruited to clean up and repair the site. The inflammatory phase usually lasts 7-10 days.
5 cardinal signs of inflammation:
- Heat
- Swelling
- Redness
- Pain
- Function loss

Retrieved 5/9/18 from: https://www.britannica.com/story/how-is-inflammation-involved-in-swelling
When does inflammation occur?
In the context of physical activity, inflammation occurs after injury or insult to the soft tissues of the body, whether that be an external object that breaks the skin, or from overuse of a limb causing unnecessary internal stretch, friction or compression of a structure, such as a tendon. For example, if you were to roll your ankle during a game of soccer, your ankle ligaments may be stretched beyond their normal limits and become torn or ruptured (i.e. spained). It is this damage that releases and activates the first inflammatory chemicals that set of the inflammatory cascade.
Causes:
- Direct blow (e.g. fall or collision with another object/person)
- Overstretching of ligaments/tendons/muscles/skin (e.g. ankle inversion injury aka ‘rolled ankle’)
- Friction (e.g. with repeated movement: tendon-on-bone, bone-on-bone)
- Penetrating object (e.g. stick through skin)
Is inflammation good or bad?
In the right context, inflammation is a good thing to an extent as it plays an important role in initiating tissue repair. Without it, it would be difficult for our tissues to repair efficiently. Rather than trying to halt the process, it is best to work to manage it appropriately.
Management:
Historically, initial treatment of soft tissue injury and inflammation has been RICE – Rest, Ice, Compression, Elevation. However, evidence has evolved to support a new acronym, MCE – Move safely, Compress, Elevate. This leaves out the need for ice, which allows the inflammatory response to work its magic, increasing oxygen-carrying blood to the area which the cells use as fuel to clear debris and repair damaged tissue. For pain relief, ice may be used immediately post injury, however, after the first hour the MCE rule should be applied.
For the same reason, it is suggested that you avoid anti-inflammatory medications (i.e. ibuprofen) during this time, instead opting for medications that work primarily to control pain.

Image retrieved 17/9/18, from: http://newhamburgwellnesscentre.blogspot.com/2013/09/rehabilitation-of-ankle-sprains_5317.html
A trained physiotherapist will help to establish safe range of movement in both the early stages, and moving forward as inflammation resolves. This helps to avoid unhelpful movement patterns as well as unnecessary stiffness and pain in the long-term, speeding up return to normal function.
LAZER (Light Amplification by Stimulated Emission of Radiation) applied by a trained physiotherapist can assist the inflammatory stage during, as the beams work to more easily dissociate oxygen bound blood cells in the damaged area, so the healing cells have access to more oxygen (fuel) and therefore can work more efficiently and effectively.

Image retrieved 17/9/18, from: https://www.djostore.com.au/chattanooga-laser-therapy-module.html
See a physiotherapist to ensure appropriate and effective management of initial inflammation and a aid a faster recovery.

10.09.2018
Lateral Hip Pain
Lateral Hip pain that can run down the outside of the leg past the knee can occur due to a multitude of pathologies but it is collectively coined as Greater Trochanteric Pain Syndrome (GTPS). The incidence of GTPS is between 1.8 and 5.6 per 1000/year making it quite a common problem. It is more common in women then men at a ratio of 4:1.
The Leap Trial which looked at the effects of three methods of treatment for GTPS was recently published in the British Medical Journal. Our clinical director Kim Snellgrove was involved in the Leap Trial as a treating physiotherapist when she worked for Alison Grimaldi in 2013/2014 and assisted with the education and exercise group.
The Leap Trial compared three groups over a 12 month period. There was a corticosteroid group, an education and exercise group and a wait and see group. At eight weeks it was found that the education plus exercise group and the corticosteroid group both reported a global improvement in their function and pain compared with the wait and see approach. The education and exercise group at 8 weeks actually performed better than the corticosteroid group. At 12 months education plus exercise showed better global improvement than the corticosteroid injection.
The education and exercise group was educated in ways to avoid compressive load to the lateral gluteal tendons. Participants posture and functional activities were corrected. Exercises involved progressive loading of the lateral gluteals commencing with a very gentle isometric program and progressing through a series of graded loaded exercises as the participant was able to tolerate the load. Reformers where also utilised in the later stage loading program in the Leap Trial.
If you are struggling with lateral hip pain at Bangalow Physiotherapy we can assist you using evidenced based rehabilitation and education.

References
Barratt, P., Brookes, N., Newson, A., Conservative treatments for greater trochanteric pain syndrome: a systematic review. British Journal of Sports Medicine 2016; 51 97-104 Published Online First: 10 Nov 2016. doi: 10.1136/bjsports-2015-095858
Grimaldi, A., Conservative management of lateral hip pain: the future holds promise http://dx.doi.org/10.1136/bjsports-2016-096600
Mellor, R., Bennell, K., Grimaldi, A., Nicolson, P., Kasza, J., Hodges, P., Wajswelner, H., Vicenzino, B., Education plus exercise versus cortisosteroid injection use versus a wait and see approach on global outcome and pain from gluteal tendinopathy: prospective, single blinded, randomised clinical trial. doi: 10.1136/bmj.k1662 | BMJ 2018;361:k1662

10.09.2018
Extracorporal Shockwave Therapy (ESWT)
What is it?
You may have heard of the new machine we have in our clinic and are wondering what it is. It is a Shockwave Machine. There are two types of Shockwave, there is radial shockwave (RSW) which we have and there is focused shock wave (FSW). Radial Shockwave is ballistically generated by compressed air. Radial Shockwave is a broad wave that can penetrate up to 5-6 cm in depth where as focused shockwave has a deeper penetration up to 12 cm. In physiotherapy radial shockwave is utilised to treat the more superficial tendons.
Shockwave is like a pressure wave and is sometimes termed an acoustic stimulator which creates biological effects.
The biological effects of shockwave are:
- Shockwave induces proliferation, migration and differentiation of stem cells, which significantly contribute to tissue healing and regeneration.
- Shockwaves promote tenocyte proliferation and progressive tendon tissue regeneration and induce biomechanical responses that promote tendon remodelling in tendinopathies.
- Bone cells are also sensitive to mechanotransduction. Shockwave enhances osteoregeneration. It can acts on the bony and periosteal cells and aids in the building of bone interacting with osteoblasts and osteoclasts. It assists in neovascularization and matrix remodelling.
- Shockwave has been shown to be a immunomodulator in wound healing and tissue regeneration mainly through anti-inflammatory strategies.
- Shockwave is also considered to be analgesic (pain relieving) due to the interference to the nervous system.
- Shockwave is not utilised with acute injuries but rather with chronic conditions that require assistance in stimulating healing. It is therefore not utilised until after 6-8 weeks of an injury.
It has been found to be beneficial in the treatment of chronic:
- Achilles Tendinopathy
- Planter Fasciitis
- Proximal Hamstring Tendinopathy
- Patellar Tendinopathy
- Adolescent Osgood Schlatters Disease
- Carpal Tunnel Syndrome
- Calcific Tendinopathy of the Shoulder
- Coccydynia
- Lateral Epicondyalgia
- Greater Trochanteric Pain Syndrome

Sazena et al found a 78.38% improvement in achilles tendinopathy after radial shockwave therapy up to one year later after 3 sessions. Combining shockwave therapy with traditional loading programs for achilles tendinopathies was found to have a significantly higher success rate than loading alone at 4 months (Rompe 2009).
Chang et al compared 12 randomized control trials and compared Focus Shockwave, Radial Shockwave and placebo. Radial Shockwave had the highest effectiveness versus placebo or Focus Shockwave in reducing pain in plantar fasciitis.
Cacchio et al utilised shockwave therapy on the chronic hamstring tendon of professional athletes and found 80% of the athletes in the shockwave group where able to return to sport after 9 weeks compared with 0% of the exercise alone group returning at 9 weeks. A greater number of participants in the shockwave group, i.e. 85 percent also reported more that a 50% reduction in pain at 3 months compared with the exercise group where only 10 % reported a 50% reduction in pain.
Patellar tendinopathy has also positively responded to radial shockwave therapy when used in combination with an eccentric training program (Van der Worp et al). Osgood-Schlatter Disease which is found in the adolescent and associated with growth spurts also effects the patella tendon. Shockwave has also been found to be of benefit with this condition (Lohrer et al).
In 2015 it was found that shockwave therapy helped reduce symptoms of Carpal Tunnel Syndrome when used in combination with night splints. There was significantly reduced pain and improved function versus the shame treatment with night splints (Wu et al).
Shockwave has also been found to be beneficial for lateral epicondylitis (tennis elbow). Lateral Epicondylitis symptoms are reported in the lateral elbow with grip and lifting. After just one treatment of shockwave at 6 months follow up grip strength and reports of pain where found to be significantly improved (Spacca et al).
Calcific Shoulder Tendinitis has also been found to benefit from radial shockwave therapy (Cacchio et al)
Most studies recommend Shockwave as an adjunct to other physiotherapy treatments. It is generally expected that shockwave will be performed 1x per week for 3-7 treatments.
References
- Aqil, A., Siddiqui, M., Solan, M., Redfern, D., Gulati, V., Cobb, J., Extracorporeal Shockwave Therapy is Effective in Treating Chronic Planterfasciitis: A Meta-analysis of RCTs.
- Cacchio., A., Paoloni., M., Barile A., Don, R., De Paulis., F., Calvisi, V., Ranovolo, A., Frascarelli., M., Santill., V., Spacca., G. Effectiveness of Radial Shock-wave Therapy for Calcific Tendinitis of the Shoulder: Single-Blind, Randomized Clinical Study. Physical Therapy 2006 May; 86(5): 672-82
- Chang, K., Chen, S., Chen, W., Tu, Y., Chien, K., Comparative Effectiveness of Focused Shockwave Therapy of Different Intensity Levels and Radial Shock Wave Therapy for Treating Plantar Fasciitis: A Systematic Review and Network Meta-analysis. Arch Phys Med Rehabil. 7/2012 93(7): 1259-68
- Cristina d’Agostino, M., Craig, K., Tibalt, E., Respizzi, S., Shockwave as biological therapeatic tool: From mechanical stimulation to recovery and healing, through mechanotransduction. Int J Surg. 11/2015
- Lohrer, H., Nauck, T., Scholl, J., Zwerver, J., Malliaropoulos, N., Extrocorporeal Shock Wave Therapy for Patients Suffering from Recalcitrant Osgood-Schlatter Disease. Sportverletz Sportschaden. 2012 Dec; 26 (4): 218-22
- Rompe, Furia, Muaffulli Eccentric Loading versus Eccentric Loading Plus Shock-wave treatment for Midportion Achilles Tendinopathy. A randomized Controlled Trial. American Journal of Sports Medicine, 2009 Vol 37, No 3 P 463-471
- Saxena, A., Ramdath, S., O’Halloran, P., Gerdesmeyer, L., Gollwitzer, H., Extra-corporeal pulsed-activated therapy for Achilles Tendinopathy: a prospective study. J Foot Ankle Surg. 2011;50(3):315-9
- Spacca, G., Necozione, S., Cacchio., A., Radial shock wave therapy for lateral epicondylitis: a prospective randomised controlled single-blind study. Eura Medicophys. 2005 Mar 41(1):17-25
- Vinding, J., Eaton, C., Shockwave Therapy in the Treatment of Musculoskeletal Disorders. DJO Publications 2016
- Van der Worp, H., Zverver, J., Hamstra, M., Van den Akker-Scheek, I., Diercks, R.L., No difference in effectiveness between focused and radial shockwave therapy for treating patellar tendinopathy: a randomized controlled trial. Knee Surg Sports Traumatol Athrosc. 2013 May
- Wu, Y., Ke M.J., Chou, Y., Chang, C., Lin, C., Li, T., Shih, F., Chen, L., Effect of radial shockwave therapy for carpal tunnel syndrome: A prospective randomized double-blind, placebo-controlled trial. J Orthop Res. 2015 Nov

What is the tendon?
The tendon is made up of strong connective tissue found at the start (origin) and finish (insertion) of a muscle connecting the muscle to the bone ultimately allowing the muscle to contract, moving the bone and creating movement. Tendons are not to be confused with ligaments, which connect bone to bone in order to stabilise joints. Both tendons and ligaments are not elastic and are capable of withstanding incredible tensions as we walk, run, dance and jump.
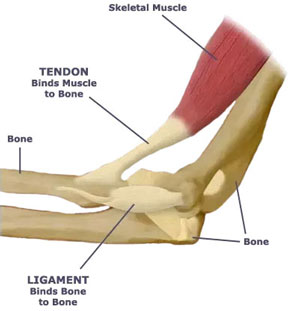
(Figure taken 15/8/18 from: https://www.quora.com/What-are-t
endons-and-ligaments-and-what-are-they-composed-of)
What is a Tendinopathy?
Tendonitis describes the condition in its early stages as inflammatory. After the initial stages, inflammation is no longer present and so the terminology of tendonitis should no longer be used. With tendinopathy, inflammation is no longer present. Instead, the tendon layout has been changed. When the tendon becomes overloaded by repetitive activities (e.g. jumping/running/hammering) or newly increased loading (e.g. increasing your running distance/pace dramatically), the fibres experience multiple microtraumas causing the release of inflammatory mediators. This causes the usually parallel-running tendon fibres to become disorganised. This disorganisation results in a newly thickened weaker tendon that is generally painful to touch and to load.
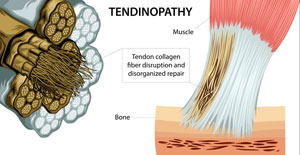
(Figure taken 29/8/18 from: http://chiroup.com/tendinopathy/)
Causes
- Repetitive activity – most often of energy storing activities (eg. jumping, running, hitting a tennis ball with a racquet, swinging a hammer)
- Increased loading
- Overuse
- Prolonged compressive force on the tendon
Signs & Symptoms
- Pain over the region of the tendon
- Pain extending into the muscle belly of the tendon
- Reduced strength
- Pain with contraction of the muscle (especially with energy storing activities)
- Tendon thickening
- Start-up pain with activity that can subside after a short amount of time during the activity
How to treat it?
Rest is not the cure – While symptoms subside during periods of rest, tendinopathies do not resolve and symptoms resume as activity resumes.
Exercise – Evidence tells us that exercise is one of the most effective way to treat a tendinopathy. Properly prescribed exercises aim to progressively load the tendon as tolerated in order to restore strength and reduce pain.
Shockwave therapy – Newly emerging evidence supports the use of shockwave therapy for stubborn tendinopathies (especially for insertional achilles and gluteus medius tendiopathies) (Al-Abbad & Simon, 2013; Rompe et al, 2009 & 2008; Rasmussen, et al, 2008)
Avoid aggravating activities. Avoid stretching.
References:
Abate M, Gravare-Silbernagel K, Siljeholm C, et al.: Pathogenesis of tendinopathies: inflammation or degeneration? Arthritis Research and Therapy. 2009, 11:235.
Al-Abbad, H., & Simon, J. V. (2013). The effectiveness of extracorporeal shock wave therapy on chronic achilles tendinopathy: a systematic review. Foot & ankle international,34(1), 33-41.
Cook J, Purdam C: Is compressive load a factor in the development of tendinopathy? British Journal of Sports Medicine. 2012, 46:163-168.
Malliaras P, Barton CJ, Reeves ND, Langberg H: Achilles and Patellar Tendinopathy Loading Programmes. Sports Medicine. 2013:1-20.
Rasmussen, S., Christensen, M., Mathiesen, I., & Simonson, O. (2008). Shockwave therapy for chronic Achilles tendinopathy: a double-blind, randomized clinical trial of efficacy. Acta orthopaedica, 79(2), 249-256.
Rompe, J. D., Furia, J., & Maffulli, N. (2009). Eccentric loading versus eccentric loading plus shock-wave treatment for midportion achilles tendinopathy: a randomized controlled trial.The American journal of sports medicine, 37(3), 463-470.
Rompe, J. D., Furia, J., & Maffulli, N. (2008). Eccentric loading compared with shock wave treatment for chronic insertional achilles tendinopathy: a randomized, controlled trial. JBJS,90(1), 52-61.

05.09.2018
Exercise Tips for Dancers
Physiotherapy Exercises
To Improve Your Pointe
Why is improving your pointe important?
When you claw or flex your toes with your
pointe you overwork the long muscle that goes
to your big toe called Flexor Hallicus Longus.
Flexor Hallicus Longus can increase in size when
overused and impinge on the inside (medial) ankle
causing pain.
“By changing your pointe to long toes
instead of flexed toes you help to avoid
irritation to the Flexor Hallicus Longus
tendon.”
If you are planning on going enpointe or are
already enpointe it also helps to reduce blistering
of the toes if you pointe with long toes in your
pointe shoes.
How To Improve Your Pointe
Pointe Range of 0-5 degrees is desirable for
dancers. Some dancers are very mobile and find
it easy to have this range whilst others may have
some restrictions that a physiotherapist could
assist with gaining.
Regardless of whether you have a very mobile
foot or restricted mobility of your pointe the
following strengthening exercises will help you
to improve your pointe technique, active mobility
and stability of your pointe and prevent injury.
Your Measured Pointe Range Is: (Pointe range
between 0-5 degrees is considered desirable).
Doming
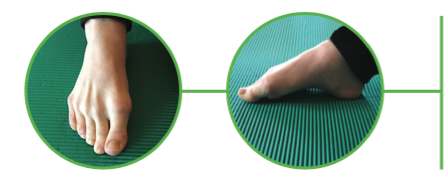
Whilst sitting on the ground place one foot on the
ground flat in front of you. Whilst keeping long toes
gently pull the arch up so as that you only flex at the
MCP joint in the foot as shown in the picture. Try to
keep the muscle at the front of the ankle called Tibialis
Anterior relaxed whilst you are doing this exercise.
Pointe Through Demi Pointe

Whilst in long sitting – start with your foot
dorsiflexed and then planterflex at the
ankle and then flex at the toes (MCP joint)
whilst maintaining long toes then return to
a dorsiflexed ankle. This exercise can also
be done with the use of a ball up against
the wall providing some resistance to the
movement.
Piano

is a toe articulation exercise that helps with awareness
of your toes and use of the small (intrinsic) muscles
found in your foot. Starting with your little toe try to
individually touch the floor with each toe until you
reach the big toe. Then go back to lifting the big toe
off first until each toe in turn is lifted off the ground
with the small toe being the last toe to lift off the
ground.
Toe Swapping
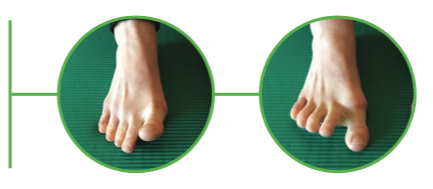
is another articulation exercise of the toes. In toe
swapping you try to lift the big toe off the ground
whilst the other toes remain stationary on the floor
and then you swap to try and lift the 4 outer toes off
the ground whilst the big toe stays on the ground and
then repeat.
Recent Comments